
Chickenpox
Did you know...
SOS believes education gives a better chance in life to children in the developing world too. A good way to help other children is by sponsoring a child
| Chickenpox | |
|---|---|
| Classification and external resources | |
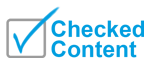
 Child with varicella disease |
|
| ICD- 10 | B 01 |
| ICD- 9 | 052 |
| DiseasesDB | 29118 |
| MedlinePlus | 001592 |
| eMedicine | ped/2385 derm/74, emerg/367 |
| MeSH | C02.256.466.175 |
Chickenpox is one of the five classical childhood exanthems or rashes, once a cause of significant morbidity and mortality, but now chiefly of historical importance. Formerly one of the childhood infectious diseases caught by and survived by almost every child, its incidence had been reduced since the introduction and use of a varicella vaccine in 1995 in the U.S. and Canada to inoculate against the disease. Other countries, such as the UK, do not mandate use of the vaccine, in part due to a lack of evidence of its efficacy.
Chickenpox is caused by the varicella-zoster virus (VZV), also known as human herpes virus 3 (HHV-3), one of the eight herpes viruses known to affect humans. It starts with conjunctival and catarrhal symptoms and then characteristic spots appearing in two or three waves, mainly on the body and head rather than the hands and becoming itchy raw pox (pocks), small open sores which heal mostly without scarring.
Chickenpox has a 10-21 day incubation period and is highly contagious through physical contact two days before symptoms appear. Following primary infection there is usually lifelong protective immunity from further episodes of chickenpox.
Chickenpox is rarely fatal (usually from varicella pneumonia), with pregnant women and those with a suppressed immune system being more at risk. Pregnant women not known to be immune and who come into contact with chickenpox may need urgent treatment as the virus can cause serious problems for the fetus. This is less of an issue after 20 weeks.
The most common complication of chicken pox is shingles; this is most frequently a late effect.
Signs and symptoms
Chickenpox is a highly contagious disease that spreads from person to person by direct contact or through the air from an infected person's coughing or sneezing. Touching the fluid from a chickenpox blister can also spread the disease. A person with chickenpox is contagious from one to two days before the rash appears until all blisters have formed scabs. This may take five to 10 days. It takes from 10-21 days after contact with an infected person for someone to develop chickenpox.
The chickenpox lesions (blisters) start as a two to four millimeter red papule which develops an irregular outline (a rose petal). A thin-walled, clear vesicle (dew drop) develops on top of the area of redness. This "dew drop on a rose petal" lesion is very characteristic for chickenpox. After about eight to 12 hours the fluid in the vesicle gets cloudy and the vesicle breaks leaving a crust. The fluid is highly contagious, but once the lesion crusts over, it is not considered contagious. The crust usually falls off after seven days sometimes leaving a crater-like scar. Although one lesion goes through this complete cycle in about seven days, another hallmark of chickenpox is the fact that new lesions crop up every day for several days. Therefore, it may take about a week until new lesions stop appearing and existing lesions crust over. Children are not to be sent back to school until all lesions have crusted over.
Chickenpox is highly contagious and is spread through the air when infected people cough or sneeze, or through physical contact with fluid from lesions on the skin. Zoster, also known as shingles, is a reactivation of chickenpox and may also be a source of the virus for susceptible children and adults. It is not necessary to have physical contact with the infected person for the disease to spread. Those infected can spread chickenpox before they know they have the disease - even before any rash develops. In fact, people with chickenpox can infect others from about two days before the rash develops until all the sores have crusted over, usually four to five days after the rash starts.
Congenital defects in babies
These may occur if the child's mother was exposed to the zoster virus during pregnancy. Effects on the fetus may be minimal in nature but physical deformities range in severity from under developed toes and fingers, to severe anal and bladder malformation. Possible problems include:
- Damage to brain: encephalitis, microcephaly, hydrocephaly, aplasia of brain
- Damage to the eye (optic stalk, optic cap, and lens vesicles), microphthalmia, cataracts, chorioretinitis, optic atrophy
- Other neurological disorder: damage to cervical and lumbosacral spinal cord, motor/sensory deficits, absent deep tendon reflexes, anisocoria/ Horner's syndrome
- Damage to body: hypoplasia of upper/lower extremities, anal and bladder sphincter dysfunction
- Skin disorders: ( cicatricial) skin lesions, hypopigmentation
Prognosis and treatment
Chickenpox infection tends to be milder the younger a child is and symptomatic treatment, with a little sodium bicarbonate in baths or antihistamine medication to ease itching, and paracetamol (acetaminophen) to reduce fever, are widely used. Ibuprofen can also be used on advice of a doctor. However, aspirin or products containing aspirin must not be given to children with chickenpox (or any fever-causing illness), as this risks causing the serious and potentially fatal Reye's Syndrome.
There is no evidence to support the effectiveness of topical application of calamine lotion, a topical barrier preparation containing zinc oxide in spite of its wide usage and excellent safety profile.
It is important to maintain good hygiene and daily cleaning of skin with warm water to avoid secondary bacterial infection. Infection in otherwise healthy adults tends to be more severe and active; treatment with antiviral drugs (e.g. acyclovir) is generally advised. Patients of any age with depressed immune systems or extensive eczema are at risk of more severe disease and should also be treated with antiviral medication. In the U.S., 55 percent of chickenpox deaths are in the over-20 age group, even though they are a tiny fraction of the cases.
Complications
Later in life, chickenpox viruses remaining dormant in the nerves can reactivate, causing shingles.
Secondary infections, such as inflammation of the brain, can occur in immunocompromised individuals. This is more dangerous with shingles.
Necrotizing fasciitis is also a well recognized lethal complication of Chickenpox, especially in children. Most important component of the management of necrotizing fasciitis is prompt and adequate surgical debridement of the lesions. So higher suspicion is very important to make the early diagnosis.
Vaccination
A varicella vaccine has been available since 1995 to inoculate against the disease. Some countries require the varicella vaccination or an exemption before entering elementary school. Protection is not lifelong and further vaccination is necessary five years after the initial immunization.
In the UK, varicella antibodies are measured as part of the routine of prenatal care, and by 2005 all NHS healthcare personnel had determined their immunity and been immunised if they were non-immune and have direct patient contact. Population-based immunization against varicella is not otherwise practiced in the UK, because of lack of evidence of lasting efficacy or public health benefit.
Vaccination reactions
Common and mild reactions following vaccination may include:
- Fever of 101.9 (38.9 C) up to 42 days after injection
- Soreness, itching at the site of injection within 2 days
- Rash occurring at site of injection anywhere form 8 to 19 days after injection. If this happens you are considered contagious.
- Rash on other parts of body anywhere from 5 to 26 days after injection. If this happens you are considered contagious.
Fever and discomfort may be lessened by taking medication containing paracetamol (aka acetaminophen, such as Panadol, Tempra, Tylenol) or ibuprofen.
History
One history of medicine book credits Giovanni Filippo ( 1510– 1580) of Palermo with the first description of varicella (chickenpox). Subsequently in the 1600s, an English physician named Richard Morton described what he thought a mild form of smallpox as "chicken pox." Later, in 1767, a physician named William Heberden, also from England, was the first physician to clearly demonstrate that chickenpox was different from smallpox. However, it is believed the name chickenpox was commonly used in earlier centuries before doctors identified the disease.
There are many explanations offered for the origin of the name chickenpox:
- Samuel Johnson suggested that the disease was "less dangerous", thus a "chicken" version of the pox;
- the specks that appear looked as though the skin was pecked by chickens;
- the disease was named after chick peas, from a supposed similarity in size of the seed to the lesions;
- the term reflects a corruption of the Old English word giccin, which meant itching.
As "pox" also means curse, in medieval times some believed it was a plague brought on to curse children by the use of black magic.
From ancient times, neem has been used by Indians to alleviate the external symptoms of itching and to minimise scarring. Neem baths (neem leaves and a dash of turmeric powder in water) are commonly given for the duration.
During the medieval era, oatmeal was discovered to soothe the sores, and oatmeal baths are today still commonly given to relieve itching.